A Smartphone Moment for Kidney Dialysis
An expert in the molecules used to develop advanced materials for aerospace, energy, and water purification, Theo Dingemans jokingly says that he “speaks polymer.” Yet some of the most memorable conversations he’s had don’t involve talking about chemical engineering with fellow scientists. He vividly recalls speaking a different type of language—one of compassion and discernment—when having conversations with kidney patients.
“Visiting the dialysis clinic was a real eye-opener, and I felt like an intruder because I’m not sick,” said Dingemans, PhD, professor and chair of the Department of Applied Physical Sciences at UNC-Chapel Hill. “Patients told me about how they were waiting for a kidney transplant, and how they had to be tied to a big dialysis machine three days a week because it keeps them alive—and when they’re done at the clinic, they go home and sleep because they’re so tired.”
Dingemans visited the clinic at the suggestion of Dr. Prabir Roy-Chaudhury, MD, PhD, the Drs. Ronald and Katherine Falk Eminent Professor in Nephrology at the UNC School of Medicine and co-director of the UNC Kidney Center. Roy-Chaudhury wanted to give Dingemans the opportunity to meet the kinds of patients whom he believes can benefit from Dingemans’ chemical engineering expertise.
Roy-Chaudhury, Dingemans and Orlando Coronell, PhD, a professor in the Gillings School of Global Public Health, have teamed up to develop a working prototype that may transform today’s large, stationary dialysis machine into a miniature, portable artificial kidney the size of a smartphone. The project is called GENESIS (Graphene Oxide Membranes for Portable Kidney Dialysis) and receives support from the UNC Institute for Convergent Science, which is part of Innovate Carolina, UNC-Chapel Hill’s initiative for innovation, entrepreneurship and economic development.

The collaborative effort hinges on development of an ultra-thin membrane technology that is roughly 100 times thinner than a human hair. If successful, the membrane may make it possible to create a wearable artificial kidney that is approximately 1,500 times smaller in volume than a standard dialysis machine. The goal is a dialysis device that straps to patients’ arms and gives them the freedom to go about their daily routines outside the clinic.
“If we can leverage this quantum jump in technology to result in miniaturization, increased efficiency and reduced cost, that’s when we will have a smartphone moment in kidney dialysis,” Roy-Chaudhury said. “By a smartphone moment, I absolutely mean superior technology at a reduced cost that improves the quality of life for millions across the globe, which is exactly what smartphones have done.”
‘Dialysis keeps you alive, but doesn’t allow you to live’
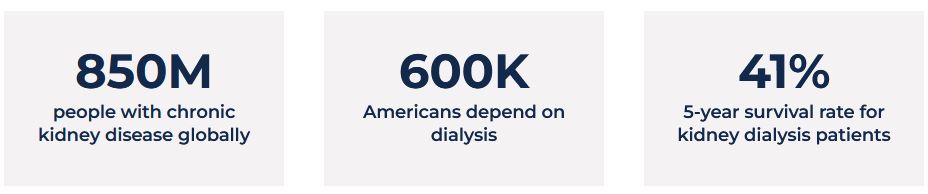
The need for innovation centers on the persistent plight of kidney patients, which Roy-Chaudhury sees routinely in his clinical work. Chronic kidney disease is one of the largest and fastest-growing global health challenges, yet it often remains underrecognized. Out of a global population of roughly 8 billion people, an estimated 850 million are living with chronic kidney disease, and its impact is expected to intensify in the coming decades. According to projections from the Global Burden of Disease Initiative, kidney disease is expected to rise from the 12th leading cause of death worldwide to the fifth by 2040. In the United States alone, about 37 million Americans—roughly one in seven adults—have chronic kidney disease.
When the disease progresses to kidney failure, patients require dialysis or a transplant to survive. Currently, about 800,000 Americans are receiving kidney replacement therapy. This includes around 250,000 people with functioning transplants and between 550,000 to 600,000 individuals (roughly 75% of patients) who depend on dialysis.
“We often say that dialysis keeps you alive, but it doesn’t allow you to live,” said Roy-Chaudhury. “Even though it allows patients to live in the short-term, the quality of life is terrible, and patients on dialysis also have a hugely increased incidence of cardiovascular disease.”
Despite decades of medical progress, modern dialysis is based on the same fundamental principles used to create the first dialysis machine over eight decades ago in 1944, and the core technology used to filter toxins from the blood has changed remarkably little since that original breakthrough. The grueling treatment produces limited outcomes: if 100 patients begin hemodialysis in the US today, only about 50 are alive after three years and just 41 after five years, Roy-Chaudhury noted. He said therapy typically requires four-hour treatments three times a week, often leaving patients exhausted and unable to do the things that they want to do.

“Our vision is that instead of being hooked up to a dialysis machine for four hours, three times per week—and feeling totally washed out for the next 10 hours after that—why can’t we build something the size of a cell phone that straps onto your arm and allows you to go about your normal day-to-day activities?”Dr. PrabirRoy-Chaudhury
The size and cost of machines also constrain progress. Today’s dialysis machines are roughly the size of a midsize refrigerator and can cost tens of thousands of dollars per unit—often between $15,000 and $35,000—requiring specialized clinic infrastructure, large volumes of purified water and trained medical staff. These limitations tether patients to the physical clinic and rigid schedules centered around their next treatment.
“Our vision is that instead of being hooked up to a dialysis machine for four hours, three times per week—and feeling totally washed out for the next 10 hours after that—why can’t we build something the size of a cell phone that straps onto your arm and allows you to go about your normal day-to-day activities?” said Roy-Chaudhury, who noted that every current standard dialysis session requires almost 200 liters of water that ultimately must be discarded as waste. “We need to leverage the best technology available to make a dialysis device that is small, portable and patient centered, runs on a couple of bottles of water, and is environmentally friendly.”
Ultra-thin membrane for miniaturizing dialysis
A few years ago, Roy-Chaudhury read an article about a water purification project Dingemans and Coronell worked on as part of the UNC Research Creativity Hubs program. The article and a suggestion made by the UNC Office of Technology Commercialization prompted him to email Dingemans to start a conversation about how innovative polymer materials might improve dialysis. Initially, Dingemans wasn’t sure if there was a connection between his lab’s work and kidney health. But as the two continued to talk, the opportunity for impact became clear.

“Prabir was persistent, and as he started explaining the challenge in kidney dialysis, I saw that there are a lot of things that my lab can contribute,” Dingemans said. “We started thinking about the membrane technologies we have, our know-how in high-performance nanocomposites, and how we could design a device that would allow us to miniaturize dialysis.”
Dingemans and Roy-Chaudhury began pulling together a team with the mix of knowledge needed to develop the membrane technology and device prototype. They enlisted the support of Coronell, an expert in membrane engineering and water purification, and Bob Geil, research assistant professor and technical director of the Chapel Hill Analytical and Nanofabrication Laboratory (CHANL), who provided expertise in building materials at an incredibly tiny nanoscale. Maruti Hegde, PhD, a research associate professor in Dingemans’ lab who specializes in next-generation polymer and nanocomposite technologies, works as a lead chemist on the project.
Coronell points to the power of combining four types of expertise: kidney dialysis knowledge (Roy-Chaudhury), membrane development (Dingemans), membrane systems (Coronell) and nano/microdevice fabrication (Geil).

“While we all bring several strengths to the project, from a big picture perspective, Prabir’s expertise on kidney dialysis provides us with clear targets on what the device we’re developing needs to deliver to improve patient outcomes,” Coronell said. “None of us individually has the expertise of the other team members, and using our four skills together will allow us to develop a membrane device that achieves those targets.”
At the heart of the GENESIS project is a new biocompatible filtration platform built from two key components: an ultra-thin membrane that performs the filtering and a supporting carrier material that allows the membrane to function inside a device. The membrane itself is made from graphene oxide–based nanocomposite materials and is extraordinarily thin—measured in nanometers and less than a micron thick, roughly ten times smaller than a human white blood cell. This extreme thinness—making the membrane almost impossible to see—is essential because the membrane must be able to filter waste products like urea from blood using only the natural blood pressure generated by the human heart. Unlike conventional dialysis systems that rely on pumps to push blood through thick filters, the GENESIS membrane is designed to operate at much lower pressures.
“For the device to be small and portable, the membrane needs to operate at the pressure of the heart, just like a regular kidney works,” explained Dingemans. “There isn’t room for us to put in a pump like membrane engineers typically do. For the membrane to work at the pressure the heart provides, we needed to make it very thin.”
Training a new generation of kidney disease researchers, advocates
Part of the support provided by ICS is its innovation postdoctoral and professional development training program, which helps postdoctoral researchers develop skills in business and technical subjects while allowing the research project team to multiply their innovation capacity in areas like technology development. Through the program, Chhabilal Regmi, PhD, a former postdoctoral researcher who worked jointly in the labs of Coronell and Dingemans, played an integral role in engineering the membrane technology and working with Geil from CHANL to build the prototype.
Undergraduate and graduate students also contribute to the GENESIS project, working across labs to bolster the cross-disciplinary effort. Inspired by her sister’s struggle with chronic kidney disease, Allegra Gray, a sophomore majoring in biomedical engineering from Dingemans’ research group, joined the project as a first-year student working in Coronell’s and Dingemans’ labs to support the team in developing the ultra-thin membranes. She’ll expand her knowledge of kidney medicine during summer 2026 after being selected to participate in the Harvard Summer Research Program in Kidney Medicine. Serving as a mentor to Gray is Maria Furukawa, a doctoral student in chemistry and member of Dingemans’ group who worked with his and Coronell’s lab team. Furukawa brings experience synthesizing liquid-crystal polymers, which possess dual solid-liquid properties that are useful for controlling the volume of water and waste that can pass through the membrane filter.

Roy-Chaudhury, Dingemans and Coronell are also part of an R25 Education Project funded by National Institutes of Health in which rising undergraduate juniors and seniors get a clinical immersion in kidney care over the summer and then participate in a research project over the next two semesters. A number of these students have chosen to work on the GENESIS project. According to Roy-Chaudhury, “What makes me really happy is that we’re not only doing cutting-edge science through this project, but we’re also developing the next generation of kidney leaders and champions.”
The membranes and prototype move to a test phase this spring, a process that will give a postdoctoral researcher and students a unique opportunity to train with dialysis technology. “We’ve created a prototype station in the ICS lab where we can test the heart of the technology, which is our membranes,” said Dingemans, who noted that the prototype will use simulated blood and water to test how effectively approximately 10 iterations of the membrane filters extract toxins while allowing necessary components such as albumin to remain in the blood. “A postdoctoral researcher will organize students who are eager to join this effort and help us collect and organize all of the data around different membrane configurations to see which ones are the winners.”
Convergence of kidney science, clinical practice draws industry interest
The collaboration between Roy-Chaudhury, Dingemans and Coronell bridges clinical practice and multiple fields of scientific research, precisely the type of cross-pollination that the Institute for Convergent Science (ICS) aims to cultivate.
ICS supports projects like GENESIS through its AGILE grant program, which provides milestone-based funding designed to help research teams move promising discoveries toward practical applications. Along the way, ICS and Innovate Carolina connect investigators with industry partners, investors and commercialization resources that can help transform early-stage ideas into technologies that benefit society.
“ICS gave us the initial ability to get together and create something that you can hold in your hand and use as the basis for intellectual property, grants and external investment,” said Roy-Chaudhury. “The convergent science funding has taken our initial dream and turned it into a physical prototype in a bricks-and-mortar setting that will help us engage with people who can fund this work.”

The ICS AGILE grant program provides seed funding for technology and prototype development and iteration. The program also offers access to project management, entrepreneurial mentors and commercialization experts, plus shared lab space where the three principal researchers, postdoctoral project leads and students can meet to iterate on prototypes and test the membranes. In the GENESIS project, the funding was generously provided through a grant to ICS from the NC Collaboratory, specifically to advance this technology.
“Before the support of ICS, all we had was an idea. The financial support ICS provided enabled us to fund personnel to develop an initial prototype of a key component of what would be a portable dialysis device, gather some initial data, and gain momentum so that we are in a position to obtain external funding to continue pursuing our goal,” said Coronell. “The laboratory space ICS provided has also been very helpful since it is located in an intermediate place between our laboratories, and we also needed the extra space for this type of collaborative work.”
“Seeing the quick and significant progress that Prabir, Theo and Orlando have made with their team and the GENESIS project in building a physical prototype for testing has been tremendously exciting,” said Greg Copenhaver, PhD, Director of the Institute for Convergent Science and Chancellor’s Eminent Professor of Convergent Science. “The GENESIS team embodies what the Institute for Convergent Science was created to support—bringing together experts from medicine, engineering, physical sciences and public health and equipping them with resources to rapidly advance bold ideas that could dramatically improve the lives of kidney patients across the U.S. and around the world.”
The project is already attracting interest from a defense-related medical entity, which holds recurring meetings with the team to track the development of the technology and determine how it might help prevent battlefield hyperkalemia or other medical issues in the future.
“One of the big problems in the battlefield is that people get crush injuries that cause muscle damage and then kidney damage that requires dialysis,” said Roy-Chaudhury. “You can imagine having a portable device that could work, even on dirty water, to dialyze those people and save their lives in the field, without needing to helicopter lift them to a major facility.”
Next-level kidney dialysis at Carolina
Military interest in innovating kidney care has historical roots that stretch back to World War II. During the war, Dutch physician Dr. Willem Kolff invented the original dialysis machine in Nazi-occupied Holland (present-day Netherlands). Dingemans, who is originally from the Netherlands, had the chance to see Kolff’s original dialysis machine when visiting the Rijksmuseum Boerhaave, located in his hometown of Leiden.


Seeing the piece of history firsthand—which Kolff built using improvised materials, including aluminum salvaged from a downed German bomber plane, a water pump from a Model T Ford and cellulose sausage casings for the filter—made an impression on Dingemans. He draws parallels in Kolff’s resourcefulness and the pull-together approach of the UNC GENESIS team.
“Kolff went out to find different types of materials, started assembling his machine and tested it,” Dingemans said. “Today, we’re doing the same thing here at UNC because, through ICS, we’re bringing together all these people from different perspectives who want to go to the next level of kidney dialysis—except now, we just have fancier tools to make it happen. We have everything here at UNC to invent the next generation of dialysis equipment.”
Looking ahead, Roy-Chaudhury emphasizes that as the technology advances, what matters most to the GENESIS team will remain constant: the patient. “Being patient centered must be the focus of how we do product development,” he said. “When you talk to patients about what’s important to them, it’s having the flexibility to travel, not being connected to a machine, not feeling washed out, and being able to do the things they actually want to do.”